Thank you to ResearchFish, a system that many UK researchers are
required to use to report their research outcomes, for providing a rich set of
examples of user experience bloopers. Enjoy! Or commiserate...
 * The ‘opening the box’ experience: forget any idea that people have
goals when using the system (in my case, to enter information about
publications and other achievements based on recent grants held): just present
people with an array of options, most of them irrelevant. If possible, hide the
relevant options behind obscure labels, in the middle of several irrelevant
options. Ensure that there is no clear semantic groupings of items. The more
chaotic and confused the interaction, the more of an adventure it’ll be for the
user.
* The ‘opening the box’ experience: forget any idea that people have
goals when using the system (in my case, to enter information about
publications and other achievements based on recent grants held): just present
people with an array of options, most of them irrelevant. If possible, hide the
relevant options behind obscure labels, in the middle of several irrelevant
options. Ensure that there is no clear semantic groupings of items. The more
chaotic and confused the interaction, the more of an adventure it’ll be for the
user.
* The conceptual model: introduce neat ideas that have the user
guessing: what’s the difference between a team member and a delegate? What
exactly is a portfolio, and what does it consist of? Users love guesswork when
they’re trying to get a job done.
* Leave some things in an uncertain state. In the case of
ResearchFish, some data had been migrated from a previous system. For this
data, paper titles seem to have been truncated and many entries only have one
page number. For example. Data quality is merely something to aspire to.
* Leave in a few basic bugs. For example, there was a point when I
was allegedly looking at page 6 of 8, but there was only a ‘navigate back’
button: how would I look at page 7 of 8? [I don’t believe page 7 existed, but
why did it claim that there were 8 pages?]
* If ‘slow food’ is good, then surely ‘slow computing’ must be too:
every page refresh takes 6-8 seconds. Imagine that you are wading through
treacle.
* Make it impossible to edit some data items. Even better: make it
apparently a random subset of all possible data items.
* Don’t present data in a way that makes it clear what’s in the
system and what might be missing. That would make things far too routine. Give
the system the apparent structure of a haystack: some superficial structure on
the outside, but pretty random when you look closer.
* Thomas Green proposed a notion of ‘viscosity’ of a system: make
something that is conceptually simple difficult to do in practice.
One form of viscosity is ‘repetition viscosity’. Bulk uploads? No way! People
will enjoy adding entries one by one. One option for adding a publication entry
is by DOI. So the cycle of activity is: identify a paper to be added; go to
some other system (e.g., crossref); find the intended paper there; copy the
DOI; return to ResearchFish; paste the DOI. Repeat. Repeatedly.
* Of course, some people may prefer to add entries in a different
way. So add lots of other (equally tedious) alternative ways of adding entries.
Keep the user guessing as to which will be the fastest for any given data type.
* Make people repeat work that’s already been done elsewhere. All my publications
are (fairly reliably) recorded in Google Scholar and in the UCL IRIS system. I
resorted at one point to accessing crossref, which isn’t exactly easy to use
itself. So I was using one unusable system in order to populate another
unusable system when all the information could be easily accessed via various
other systems.
 * Use meaningless codes where names would be far too obvious. Every
publication has to be assigned to a grant by number. I don’t remember the
number of every grant I have ever held. So I had to open another window to
EPSRC Grants on the Web (GOW) in order to find out which grant number
corresponds to which grant (as I think about it). For a while, I was working from
four windows in parallel: scholar, crossref, GOW and ResearchFish. Later, I
printed out the GOW page so that I could annotate it by hand to keep track of
what I had done and what remained to be done. See Exhibit A.
* Use meaningless codes where names would be far too obvious. Every
publication has to be assigned to a grant by number. I don’t remember the
number of every grant I have ever held. So I had to open another window to
EPSRC Grants on the Web (GOW) in order to find out which grant number
corresponds to which grant (as I think about it). For a while, I was working from
four windows in parallel: scholar, crossref, GOW and ResearchFish. Later, I
printed out the GOW page so that I could annotate it by hand to keep track of
what I had done and what remained to be done. See Exhibit A.
* Tax the user’s memory: I am apparently required to submit entries
for grants going back to 2006. I’ve had to start up an old computer to even
find the files from those projects. And yes, the files include final reports
that were submitted at the time. But now I’m expected to remember it all.
* Behave as if the task is trivial. The submission period is 4 weeks.
A reminder to submit was sent out after two weeks. As if filling in this data
is trivial. I reckon I have at least 500 outputs of one kind or another. Let’s say 10 minutes per output (to
find and enter all the data and wait for the system response). Plus another
30-60 minutes per grant for entering narrative data. Yay: two weeks of my life
when I am expected to teach, do research, manage projects, etc. etc. too. And that assumes that it’s easy to organize
the work, which it is not. So add at least another week to that estimate.
 * Offer irrelevant error messages: At one point, I tried doing a
Scopus search to find my own publications to enter them. Awful! When I tried
selecting one and adding it to my portfolio, the response was "You are not
authorized to access this page.” Oh: that was because I had a break between
doing the search and selecting the entry, so my access had timed out. Why
didn’t it say that?!?
* Prioritise an inappropriate notion of security over usability: the security risk of leaving the page unattended was infinitesimal, while the frustration of time-out and lost data is significant, and yet researchfish timed out in the time it took to get a cup of coffee. I suspect the clock on the researchfish page may have been running all the time I was using the Scopus tool, but I'm not sure about that, and if I'm right then that's a crazy, crazy was to design the system. This kind of timeout is a great way of annoying users.
* Offer irrelevant error messages: At one point, I tried doing a
Scopus search to find my own publications to enter them. Awful! When I tried
selecting one and adding it to my portfolio, the response was "You are not
authorized to access this page.” Oh: that was because I had a break between
doing the search and selecting the entry, so my access had timed out. Why
didn’t it say that?!?
* Prioritise an inappropriate notion of security over usability: the security risk of leaving the page unattended was infinitesimal, while the frustration of time-out and lost data is significant, and yet researchfish timed out in the time it took to get a cup of coffee. I suspect the clock on the researchfish page may have been running all the time I was using the Scopus tool, but I'm not sure about that, and if I'm right then that's a crazy, crazy was to design the system. This kind of timeout is a great way of annoying users.
* Minimise organization of data: At one point, I had successfully found
and added a few entries from Scopus, but also selected a lot of duplicate
entries that are already in Researchfish. There is no way to tell which have
already been added. And every time the user tries to tackle the challenge a
different way it’s like starting again because every resource is organized
differently. I have no idea how I would do a systematic check of completeness
of reporting. This is what computers should be good at; it’s unwise to expect
people to do it well.
* Sharing the task across a team? Another challenge. Everything is
organised by principal investigator. You can add team members, but then who
knows what everyone else is doing? If three co-authors are all able to enter
data, they may all try. Only one will succeed, but why waste one person’s time
when you can waste that of three (or more) people?
* Hide the most likely option. There are several drop-down menus
where the default answer would be Great Britain / UK, but menu items are
alphabetically ordered, so you have to scroll down to state the
basically-obvious. And don’t over-shoot, or you have to scroll back up again.
What a waste of time! There are other menus where the possible dates start at 1940: for reporting about projects going back to 2006. That means scrolling through over 60 years to find the most probable response.
* Assume user knowledge and avoid using forcing functions: at one
point, I believed that I had submitted data for one funding body; the screen
icon changed from “submit” to “resubmit” to reinforce this belief. But later someone
told me there was a minimum data set that had
to be submitted and I knew I had omitted some of that. So I went back and
entered it. And hey presto: an email acknowledgement of submission. So I hadn’t
actually submitted previously despite what the display showed. The system had
let me apparently-submit without blocking that. But it wasn’t a real
submission. And even now, I'm not sure that I have really submitted all the data since there is still an on-screen message telling me that it's still pending on the login page.

 *Do not support multi-tasking. When I submitted data for one funding body, I wanted to get on with entering data for the next. But no: the system had to "process the submission" first. I cannot work while the computer system is working.
*Do not support multi-tasking. When I submitted data for one funding body, I wanted to get on with entering data for the next. But no: the system had to "process the submission" first. I cannot work while the computer system is working.
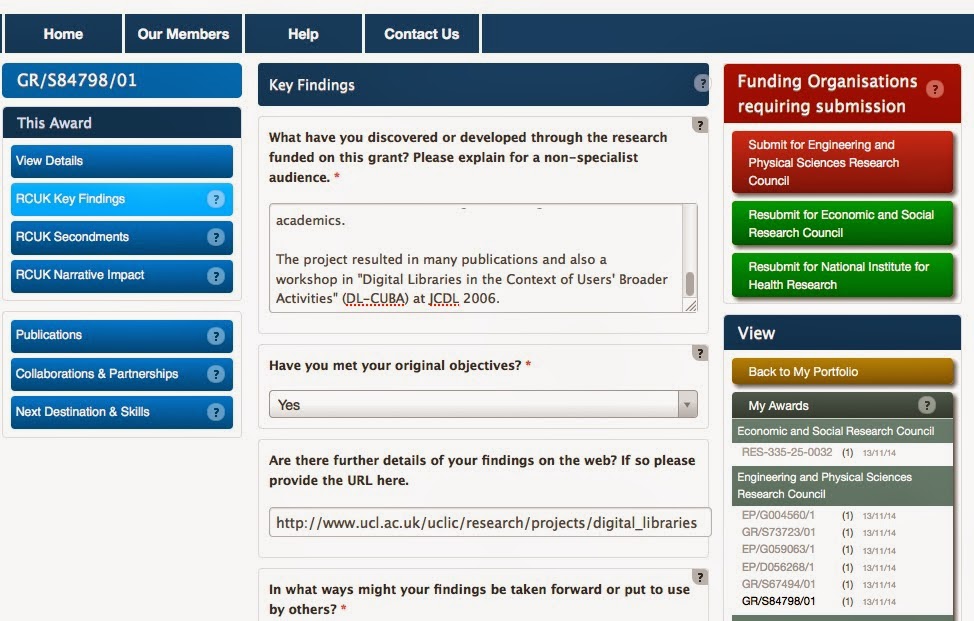
* Entice with inconsistency. See the order of the buttons for each of several grants (left). Every set is different. There are only 6 possible permutations of the three links under each grant heading; 5 of them are shown here. It must take a special effort to program the system to be so creative. Seriously: what does this inconsistency say about the software engineering of the system?
* Add enticing unpredictability. Spot the difference between the two screen shots on the right. And then take a guess at what I did to cause that change. It took me several attempts to work it out myself.
I started out trying to make this blog post light-hearted, maybe even amusing. But these problems are just scratching the surface of a system that is fundamentally unusable. Ultimately I find it really depressing that such systems are being developed and shipped in the 21st Century. What will it take to get the fundamentals of software engineering and user experience embedded in systems development?
 Last week, my car gained a puncture. On a Sunday. Not a good experience. But sorting out was as painless as I can imagine: it was quick to find a mobile tyre replacement service (etyres, in case anyone else suffers a similar fate), to identify a suitable tyre amongst a very large number of options and to fix a fitting time. All online (apart from the actual fitting, of course), and all clear and simple. It just worked.
Last week, my car gained a puncture. On a Sunday. Not a good experience. But sorting out was as painless as I can imagine: it was quick to find a mobile tyre replacement service (etyres, in case anyone else suffers a similar fate), to identify a suitable tyre amongst a very large number of options and to fix a fitting time. All online (apart from the actual fitting, of course), and all clear and simple. It just worked.